
Hypertension, Asymptomatic Hypertension, and Time to Relax
Introduction
Hypertension is one of the most common diagnoses in the United States, with nearly half of US adults having hypertension in some form and hypertension contributing to over 500k excess deaths yearly (CDC, 2025). Hypertension is a significant contributor to other leading causes of death, including vascular diseases, heart disease, strokes, and kidney disease. Good hypertension control to this day remains one of the pillars of both emergency and family medicine, and having a good understanding of hypertension, its risks, and its role in emergency medicine is important.
What is hypertension?
Hypertension (HTN) is defined as any consistent blood pressure reading >140/90 by the AHA (Vidal-Petiot, 2022). It is categorized into stages, with stage 1 hypertension being 130-139/80-89 and stage 2 hypertension beginning at >140/90 (Vidal-Petiot, 2022). Patients with stage 2 hypertension are most commonly given some kind of blood pressure medication for home management, with first line treatments including oral beta blockers, ACE inhibitors, and thiazide diuretics (especially with heart failure patients).
Hypertension is called the silent killer because most patients remain almost entirely asymptomatic as hypertension progresses. Many of our patients walk around with significant hypertension on a daily basis with no idea that something is wrong.
What Hypertension Does to Our Vessels
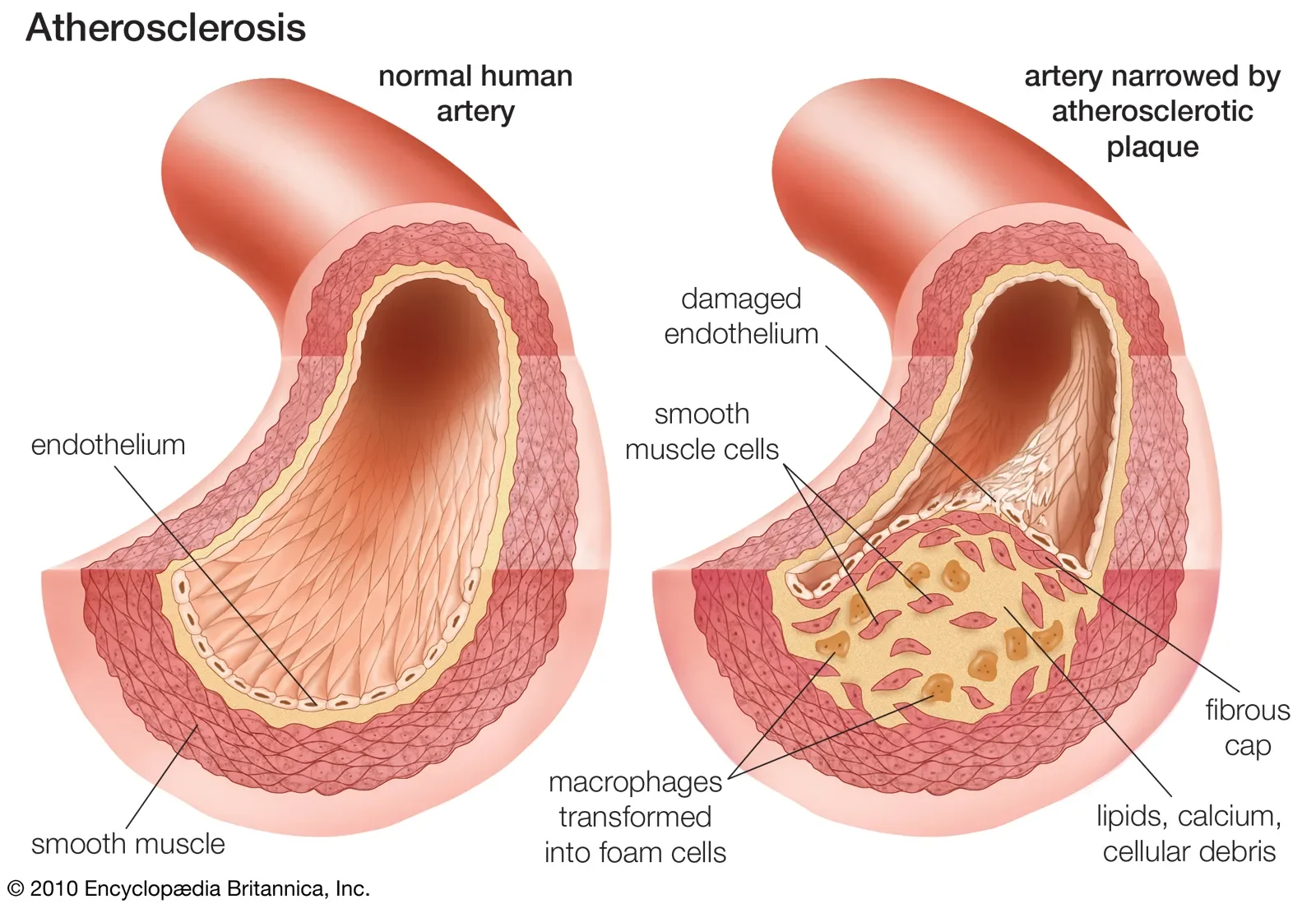
The body does well at compensating for blood pressure changes in acute situations such as exercise or transient periods of stress, but with time the force of excessive blood pressure against the veins can degrade our vasculature. The endothelium, which is the innermost layer of blood vessels and actually makes contact with blood as it flows through circulation, becomes degraded and damaged on a micro level with long-term hypertension. The endothelium, in addition to being the actual physical layer inside the vessels, is also chemically active. In response to physiological changes such as stress, infection, or (you guessed it) hypertension, the endothelium senses changes and releases mediators that either induce vasoconstriction or vasodilation of the smooth muscle.
While the exact mechanisms are complex and not totally known, long term hypertension induces a process called vascular remodeling that results in arteriosclerosis, stiffening of the arteries, and both reduced lumen and outer vessel diameter (Intengan & Schiffrin, 2001). There is both eutrophic hypertrophy of the vessel in which the actual lumen becomes smaller as vascular remodeling causes inward growth, and hypertrophic remodeling in which the outer diameter of the vessel itself becomes thicker, reducing potential space inside the vessel as a result (Rizzoni et al., 2022). Collagen production and implantation increases in the vessel walls, worsening the vessel’s ability to flex and relax to lower pressures. This raises the vessel’s natural resistance to blood flow and lowers vascular compliance, which in turn makes it so that the body must maintain higher pressures in order to flow the same amount of volume to maintain perfusion. This is a positive feedback loop that will require lifestyle intervention and pharmacological management to reduce and prevent.
With time, hypertension causes microvascular damage that will damage perfusion to our tissues in all parts of the body. For example, the nephrons, the functional units of the kidneys, are extremely sensitive to pressure changes. With chronic high pressures, these nephrons become damaged and have reduced perfusion, which in turn reduces their ability to filter the blood and produce urine. This in time causes renal disease and failure.
Afterload is a core concept to understand when discussing hypertension. Afterload is the pressure that the left ventricle must flow against in order to circulate blood through the aorta and to the rest of systemic circulation. In other words, it is the resistance that the body gives against the left ventricle. The heart in turn has to increase contractility and raise its own pressure to overcome excessive afterload, which will in turn worsen hypertension and induce a positive feedback loop.
Another core concept to understand is systemic vascular resistance (SVR) which is the passive resistance of the peripheral vasculature against inflow to them. High degrees of vasoconstriction will increase SVR, essentially making the blood vessels “tighter” and harder to flow through and producing higher end pressures. This is a core component of afterload. Examples of causes of elevated SVR include sympathomimetic use such as cocaine, chronic blood vessel changes from prolonged hypertension and arteriosclerosis, age-related elasticity loss, and excessive stress.
While this sounds complicated, it is truly just a matter of physics. A high pressure fluid (blood) flowing through a tube (blood vessel) is growing to at first stretch the vessel (elasticity), and with time worsen its elasticity. As the vessel becomes less elastic and more rigid, higher pressures are needed to achieve the same total volume at the same rate of speed. This makes the hypertension worse!
Acute Hypertension Issues
Hypertensive emergency is defined as significant systolic hypertension with evidence of end organ damage present. It typically is seen over 180/120 mmhg (BMJ, 2026). Examples of end organ damage include new-onset renal failure or damage with decreased urine output, altered mental status, and SCAPE respiratory distress. Hypertensive emergency can also induce cardiac ischemia and elevated troponin, as the heart primarily perfuses itself during diastole (and if diastole does not allow for adequate filling, then the heart is starved of blood!) Hypertensive emergency requires rapid identification and correction to prevent further damage.
Hypertensive urgency is a blanket term for blood pressure that is concerning but is not causing acute end organ damage. This is typically diagnosed in patients with pressures exceeding 180/120mmhg.Its actual definition and diagnosis remain disputed, and the term itself is moreso used to refer to blood pressures that we should probably address sooner rather than later but do not pose an imminent life threat like hypertensive emergency does.
Cerebral Autoregulation & Autoregulation
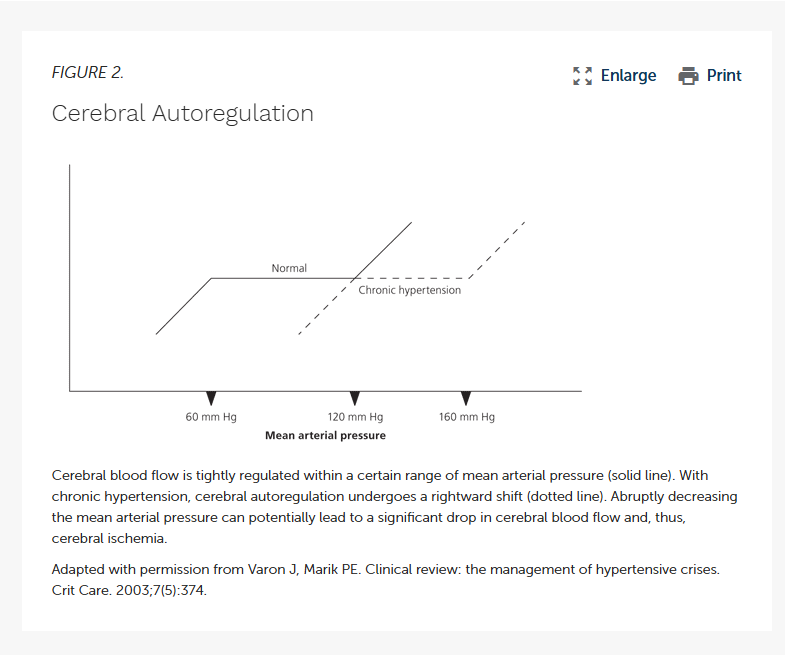
The brain is both extraordinarily resource-intensive to perfuse and extraordinarily sensitive to changes in blood flow. It requires constant, consistent, continuous blood flow to maintain perfusion. The body maintains cerebral perfusion at all times through cerebral auto regulation, which is the brains way of compensating to fluctuations in mean arterial pressure by either vasodilating or vasoconstricting the cerebral vasculature. The brain is especially sensitive to changes in continuous blood flow (CBF) and has to maintain a constant flow at all times, which requires the vessels to proactively and constantly respond to changes in pressure minute by minute. Drops in pressure, such as with orthostatic hypotension, are not acceptable for the brain (that’s why we lose consciousness in orthostatic postural hypotension!)
Cerebral perfusion pressure is dictated by the difference of MAP - ICP (intracranial pressure). The difference is the cerebral perfusion pressure. If ICP is high, MAP raises.
Hypertension: The Big Deal?
Hypertension is, of course, something that must be managed and addressed in an appropriate and safe manner. However, we must be cognizant of the patient’s whole health picture and not merely treat numbers on a screen. Patients that come in hypertensive - either to the ED or in EMS - that are without another underlying HTN-causing issue are often baseline hypertensive. Think of your classic hypertensive patients that run out of their medications, have no access to meds, or just simply have a multitude of chronic health issues; these patients are likely routinely hypertensive on a daily basis. As a result, their cerebral autoregulation has adapted to maintain blood flow at this level of blood pressure. These patients actively maintain this blood pressure to keep perfusion going without disruption.
Hypertension is a chronic, not an acute problem. There is no true “impending stroke” level blood pressure as we commonly see popularized in TV shows, media, and amongst our well-intentioned colleagues. The vessels are not merely waiting for the number to hit a certain point and then burst (and if they are, there are bigger issues in the first place). An otherwise stable and healthy patient that has hypertension is simply that in the absence of other complications. Exemptions to this include those with end organ damage signs or those with significant risk factors such as a previous aneurysm diagnosis.
By intervening with asymptomatic HTN, we risk disrupting the mean arterial pressures that they have become accustomed to, dropping it excessively, and thus causing a risk of cerebral hypoperfusion. In addition, invasive blood pressure medications are both hard to titrate according to the individual patient and easy to overshoot, and the process of titrating safely can be excessively long when it is unnecessary in the first place.
Current ACEP guidelines endorse leaving management of asymptomatic hypertension to primary care providers in the outpatient setting rather than acute intervention (Gemme, 2025).
A Note on Nursing Transfer to the Floor
As stated above, management of asymptomatic HTN is an issue that is, for safety reasons, best left to outpatient primary care providers rather than an acute emergency department issue. Even in the admitted patient, it is not necessary to rapidly control and lower blood pressures. For many of these patients being admitted, hypertension is a secondary issue rather than something to acutely address. Therefore, blood pressure is no real reason to avoid transfer to the floor if the patient is otherwise stable and resuming their own antiHTN medications. ICU beds and intermediate levels of care are much better suited to be given to patients with more critical issues than patients with merely out of range blood pressures and no other underlying issues.
References
BMJ. (2026, March). Hypertensive emergencies - Symptoms, diagnosis and treatment | BMJ Best Practice US. https://bestpractice.bmj.com/topics/en-us/27
Gemme, S. (2025, June 25). ACEP Clinical Policy on Outpatient Mgmt. of Adults with Asymptomatic Elevated Blood Pressure - ACEP Now. ACEP Now. https://www.acepnow.com/article/acep-clinical-policy-on-outpatient-mgmt-of-adults-with-asymptomatic-elevated-blood-pressure/
Intengan, H. D., & Schiffrin, E. L. (2001). Vascular remodeling in hypertension. Hypertension, 38(3), 581–587. https://doi.org/10.1161/hy09t1.096249
Kessler, C. S., & Joudeh, Y. (2010, February 15). Evaluation and treatment of severe asymptomatic hypertension. AAFP. https://www.aafp.org/pubs/afp/issues/2010/0215/p470.html?
Rizzoni, D., Agabiti-Rosei, C., & De Ciuceis, C. (2022). State of the Art review: Vascular Remodeling in Hypertension. American Journal of Hypertension, 36(1), 1–13. https://doi.org/10.1093/ajh/hpac093
Vidal-Petiot, E. (2022). Thresholds for hypertension definition, treatment initiation, and treatment targets: Recent Guidelines at a glance. Circulation, 146(11), 805–807. https://doi.org/10.1161/circulationaha.121.055177